
Cognitive Questions?
PODIATRYPREP.org
(c) All rights reserved, USA.
Foot and Ankle Research Consortium, Inc.
SAMPLE QA
[Surgical/Medical Case Structured Interrogatives – CBPS]
COGNITIVE CBPS QUESTIONS 2.0
[WHAT THEY ARE – HOW THEY WORK]
We are often asked about the difference between the mere “rote memory” QAs of the past and the modern day “cognitive” styled QAs that are currently emerging on all board examinations. NOTE [AKA: CBPS, CBT, CPC, EBM, MCQS and COGNITIVE QUESTIONS with RRA material, etc].
And so – assuming you are educated and completed podiatric medical school and did some sort of residency training [1-4 years], internship, fellowship or preceptorships – the next step in demonstrating united didactic and clinical knowledge is to pass new-wave board examination questions like the one below. Thus, our theoretical goal is not to educate you -BUT- to pragmatically help you pass modern podiatric board exam tests.
This can be accomplished on a Computer Based Testing [CBT] platform with traditional distractors [1-5 multiple-choice] -OR- by actually typing in sentences and paragraphs of response [250 words] -OR- by selecting among distractors that are several paragraphs long -OR- by speaking into a voice recorder -OR- through a combination of all styles.
So, beware! This difference is our differentiator and your path to board certification exam success both now and into the future.
CASE STUDY: Clinical Presentation
A 35 year old male with right foot pain and is 2 years post-op bunionectomy. Patient has a hallux varus deformity, ask for clinical photograph. X-rays show a staked medial metatarsal head, fibular sesamoid removed, IM, PASA, and DASA are WNL. Clinical observation shows a tight medial capsule and hyperactivity of the abductor hallucis and a partially reducible deformity. Discuss the etiology of hallux varus and the soft tissue and bone treatments.
Review:
Hallux varus can be considered an iatrogenic complication of hallux valgus surgery. There are many causes of hallux varus, including excessive lateral release, spiking of the first metatarsal (excess removal of the first metatarsal head or base of the proximal phalanx), lateral sesamoid removal, creation of a negative PASA, IM angle or over plication of the medial capsule.
Hallux varus is one of the most frustrating complications of bunion surgery because of moderate to severe dysfunction and the necessity in many cased for reoperation, including soft tissue procedures, reosteotomy, joint ablative procedures, or implant arthroplastic procedures. The surgeon should be aware, on the initial X-ray, of a potential hallux varus. This is usually noted by:
1. Peaking medial sesamoid [excess removal articular surface epicondyle staking metatarsal head].
2. Fibular sesamoidectomy.
3. Negative IM angle or PASA.
4. Varus attitude of the hallux.
5. Grade I is a 20 degree medial deviation which is completely reducible and usually occurs within the first six months of surgery.
Grade II is a 30 degree medial deviation with mild hallux flexus which is reducible and usually occurs within 12 months of surgery.
Grade III is a 30 degree varus attitude of the hallux with hallux flexus, contraction of the long extensor tendon, which is non-reducible in nature and may occurs after 12 months of initial operation.
Treatment of hallux varus is time-related and usually begins non-operatively although, in some cases when a severe hallux varus is noted, reoperation may be then procedure of choice within the first 3-6 weeks. In most instances, however, non-operative therapy should be utilized and this includes valgus strapping of the great toe, physical therapy to abduct the great toe, stretching of the contracted medial capsule, and valgus splint and pointed shoes to help decrease the potential problem. A trial of non-operative therapy lasting at least 6-8 weeks would be initiated before reoperation is proposed.
Operations for hallux varus fall into four categories: soft tissue release, re-osteotomy to realign joint surfaces, arthro-plastic resections with or without implants and fusion procedures.
Soft Tissue Release:
This is usually indicated in a Grade I with 20 degrees or less medial deviation, which is completely reducible in nature.
Goals of soft tissue release:
1. T-shaped release of the medial capsule.
2. Lateralization of the long extensor tendon.
3. Complete medial release of tibial sesamoid except for the inter-sesamoidal ligament.
4. Complete soft tissue release of first metatarsal head and lateral aspect of first metatarsal head to midshaft of bone.
5. Temporary K-wire fixation through first metatarso-phalangeal joint for 3-4 weeks.
6. Intensive post-operative rehabilitation with physical therapy, swelling control, and abduction splinting. Care must be taken not to over-correct the release, or the hallux valgus will reoccur.
When the varus has been present for six months or more, 30 degrees of medial deviation of the hallux may occur with mild flexion of the distal interphalangeal joint with extensor contracture and the ability to completely reduce the deformity.
1. Complete soft tissue release including complete medial release, lateralization of the extensor tendon, tibial sesamoid release. If there is excessive flexion of the distal inter phalangeal joint with extensor contracture, then the possibility of an inter phalangeal hallux fusion must be considered.
2. Re-osteotomy of the first metatarsal if necessary. In Grade III hallux varus, there is usually a non-reducible deformity with 30 degrees or more of medial deviation and moderate to severe hallux flexus with extensor contracture and stiffness of the joint.
Reduction of Grade III hallux varus should proceed as follows:
1. Complete soft tissue release as described above.
2. If this is a fairly young patient with necessity for functional demands on the foot, opening osteotomy of the distal first metatarsal with reangulation of the articular surface is the procedure of choice. This procedure can be performed in a variety of methods, including the reverse Austin, reverse Reverdin, or Z-osteotomy, increasing the proximal articular set angle. In addition, extensor lengthening with IP fusion may be the procedure of choice.
3. When there is arthrosis of the first metatarso-phalangeal joint, prosthetic implantation may be considered. If an IPJ fusion is necessary, however, the procedure becomes much more difficult due to the amount of bone needed to successfully seat the hemi or distal end of the hinge implant. In cases of severe recurrent hallux varus, fusion is the procedure of choice.
ANGULAR RELATIONSHIPS IN HALLUX ABDUCTO VALGUS DEFORMITY
1. Specific weight bearing angular measurements for determination HV severity.
a. Metatarsus adductus angle. Shows the positions of the metatarsals in relation to the lesser tarsus, and is important in the evaluation of the hallux valgus deformity for two reasons:
1. An increased metatarsus adductus angle has a higher susceptibility to hallux valgus formation.
2. An increased metatarsus adductus angle will cause a relative increase in the inter-metatarsal angle resulting in radiologic miscalculation of the intermetatarsal angle.
2 Metatarsus Primus Adductus Angle – Intermetatarsal angle. The relationship of a line bisecting the 1st and 2nd metatarsal shafts: normal = 8-10 degrees – avg. 8.5.
3. First MPJ position
Determined by a comparison of a line representing the effective articular cartilage of the base of the proximal phalanx and that of the head of the 1st metatarsal.
a. Congruous joint – Lines drawn are parallel to each other – Ideal joint.
b. Deviated joint – Lines drawn intersect outside the joint spaces – Phalanx is deviated without base being displaced off the metatarsal head.
c. Subluxed joint – Lines drawn intersect within the joint space – Proximal phalanx base is not completely articular with 1st metatarsal head.
d. Dislocated joint – Base of proximal phalanx in different plane than that of first metatarsal head – Proximal phalanx base is not articulating with first metatarsal head.
4. Hallux Abductus Angle
The relationship of a line representing the bisection of the longitudinal axis of the shaft of the proximal phalanx and of the 1st metatarsal: normal 10-15 degrees.
5. Proximal Articular Set Angle (PASA)
Angle formed by the relationship of a line drawn representing the effective articular surface of the 1st metatarsal head and a line perpendicular to a line bisecting the shaft of the 1st metatarsal: normal up to 8 degrees.
6. Hallux Interphalangeal Angle
Line representing the bisection of the shaft of the proximal phalanx in relationship to a line representing the bisection of the distal phalanx: normal = 0-10 degrees.
7. Distal Articular Set Angle (DASA)
Angle formed by a line drawn perpendicular to the effective articular cartilage of the base of the proximal phalanx and a line representing the longitudinal bisection of the proximal phalanx: norm up to 8 degrees.
8. Tibial sesamoid position
a. Relationship of tibial sesamoid to the longitudinal bisection of the shaft of the 1st metatarsal.
b. There are 7 positions from medial to lateral:
c. Position 3 is regarded as normal
9. Metatarsal Protrusion Distance
a. The relationship between the length of the 1st and 2nd metatarsals.
b. The bisection of the 1st metatarsal is extended proximally to intersect the bisection of 2nd metatarsal.
c. A compass is placed at the point of intersection and then set to the length of each metatarsal head, at which time an arc is created for each. The distance between the arc is the difference between metatarsal length, a (+) mm distance indicates 1st metatarsal is longer than the second.
10. Axial Sesamoid View
This projection is taken specifically to ascertain the position of the medial sesamoid in relation to the plantar crista. The medial sesamoid may actually ride over the crista without grinding it off in many cases. The severity of the bunion seems to increase when the sesamoid is lateral to the crista.
11. The Lateral View
This projection is important to measure the average metatarsal declination which approaches approximately 21 degrees and any midtarsal faults of cyma line deviations which may be present.
12. Joint Assessment
Overall assessment of metatarsophalangeal joint. Abnormalities such as cyst formation, erosions, osteophyte formation, both on the A/P and lateral views and cartilage defects should be noted.
a. A positional deformity is one in which the sum of the proximal articular set angle and the distal articular set angle is less than the hallux abductus angle.
b. A structural deformity is the sum of the proximal and distal articular set angles, which equal the hallux abductus angle.
c. Combined: When the joint is deviated or subluxed and the sum of the proximal articular set angle and distal articular set angle is less than the hallux abductus angle.
LaPorta has described numerical comparisons to determine whether the hallux valgus deformity was positional (soft tissue) or structural in nature. Haas ascertained that there were three types of metatarsal heads which are present.
a. A round metatarsal head, which is the most unstable
b. A square metatarsal head – more stable, but more amenable to hallux limitus.
c. A square metatarsal head with a central ridge, which seems to be the most stable, but also may be associated with hallux limitus or rigidus
FIRST METATARSOPHALANGEAL JOINT ARTHRODESIS
There have been a variety of procedures utilized to fuse the first metatarsophalangeal joint. These include McKeever’s procedure, as well as procedures advocated by Johannson and Barrington and Wilson. The classic McKeever arthrodesis, with a modification as noted by Lipscomb and advocated by Mann, may be the technique of choice.
Indications:
1. Severe rheumatoid hallux valgus.
2. Iatrogenic hallux varus.
3. Post-Keller procedure.
4. Hallux valgus in spastic cerebral palsy.
5. Hallux rigidus and recurrent hallux valgus deformity.
A midline incision from the midshaft of the proximal phalanx to the midshaft of the first metatarsal phalangeal joint. Medial capsulotomy is performed and excessive degloving of the metatarsal phalangeal joint is avoided.
The osteotomy is performed with minimal bone resection. The final result should have at least 15-25 degrees of dorsiflexion on the sagittal plane as well as 10-20 degrees of valgus attitude on the transverse plane.
Two Steinman pins of at least 9/64″ or one Steinmann pin at least 1/8″ in diameter is recommended. These pins are threaded and should be left in place at least 12 weeks or until bony fusion is noted. It is important to use as large a threaded Steinman pin as possible. Because of ambulation, the patient may break these pins into 3-4 pieces resulting in loss of stability. Screw arthrodesis is utilized in non-rheumatoid patients and is inserted according to the Lipscomb technique from the medial plantar surface of the base of the proximal phalanx into the metatarsal. Non-weightbearing for 8-14 weeks until fusion has taken place. Therapy and shoe fitting is indicated, with possible arch support if necessary.
Complications:
1. Failure to dorsiflex and abduct the hallux, resulting in a hyperextended gait with associated functional difficulties.
2. Non-union in the 5-10% range.
3. Interphalangeal arthritis rate of 10%.
4. Fracture of the Steinman pins. This occurs when small threaded Kirschner wires utilized instead of Steinman pins. Migration is possible.
5. Extreme shortening of the fusion site, resulting in adduction of lesser toes with pain and deformity.
6. Hyperextension of the hallux upon fusion, causing distal toe pain and extreme shoe irritation during gait.
***
ADDITIONAL BRIEF SAMPLE
***
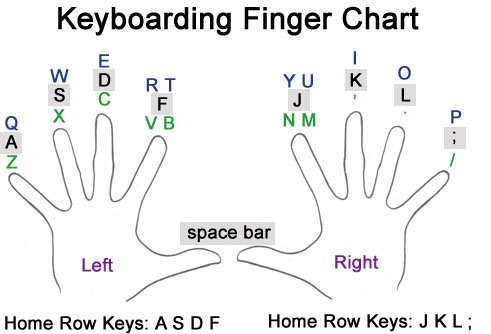
BRUSH UP ON TYPING AND KEY-BOARDING SKILLS?
[Be prepared to type 250 word responses for deeper cognitive knowledge Q&As]
BOARD PREPARATION – REDEFINED®
***
***
If you want medical education – try a seminar!
If you want to “pass the modern boards” – try us!
***
WE ARE PODIATRY PREP.org
![]()
